SPECT-CT Knee Imaging Protocol, Interpretation, and Indications
What follows is my own imaging protocol which may be different from other centres.
An injection of a Tc99m phosphate compound is followed by a dynamic acquisition of both knees and blood pool phase imaging.
We have recently started performing SPECT-CT during the blood pool phase instead of planar imaging.
Whole body planar images are performed after 3 hours, which are important to evaluate for other sites of joint disease aside from the knees.
Finally, a delayed phase SPECT-CT of both knees is performed. Our CT scans are performed with an extended Hounsfield scale to reduce metallic artefact.
We perform long length CT topograms from the pelvis to ankles to assess component position and leg length. This has the advantage of reduced radiation doses from the CT compared to the Perth CT protocol. The femoral and tibial components should be orientated perpendicular to the mechanical axis. Antero-posterior angulation of the femoral component and posterior tilt of the tibial component can also be assessed from these topograms.
Rotation of the femoral component can be assessed on CT by measuring the angle between the posterior aspect of the condylar component with a line drawn between the prominence of the lateral epicondyle and sulcus of the medial epicondyle (also known as the transepicondylar line). There are several methods for measuring the rotation of the tibial component, but the most commonly used has been described by Berger as the angle between the anterior aspect of the tibial component and the medial two-thirds of the tibial tuberosity.
Aseptic Loosening
Aseptic loosening is physical movement of the prosthesis and is due to a number of causes.
- Poor initial positioning of the prosthesis,
- Material failure of the prosthesis,
- Reaction between the bone and a component of the prosthesis causing osteolysis of bone.
Always compare the SPECT-CT with a baseline plain film from surgery. Movement of the prosthesis on serial imaging indicates loosening, and a SPECT-CT adds little aside from identifying infection. SPECT-CT is useful in evaluating the bone stock prior to revision surgery. When previous imaging is not available, or findings are equivocal, then SPECT-CT can have a high degree of accuracy for identifying loosening.
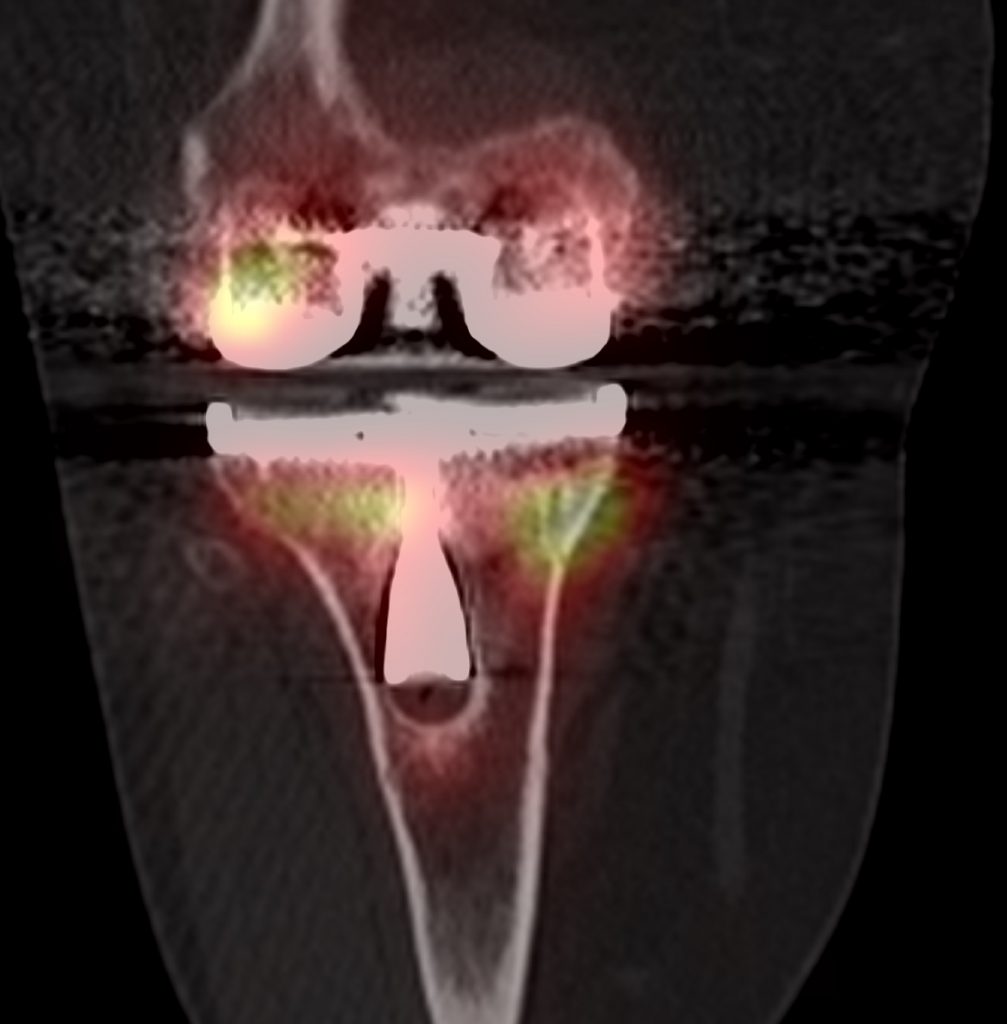
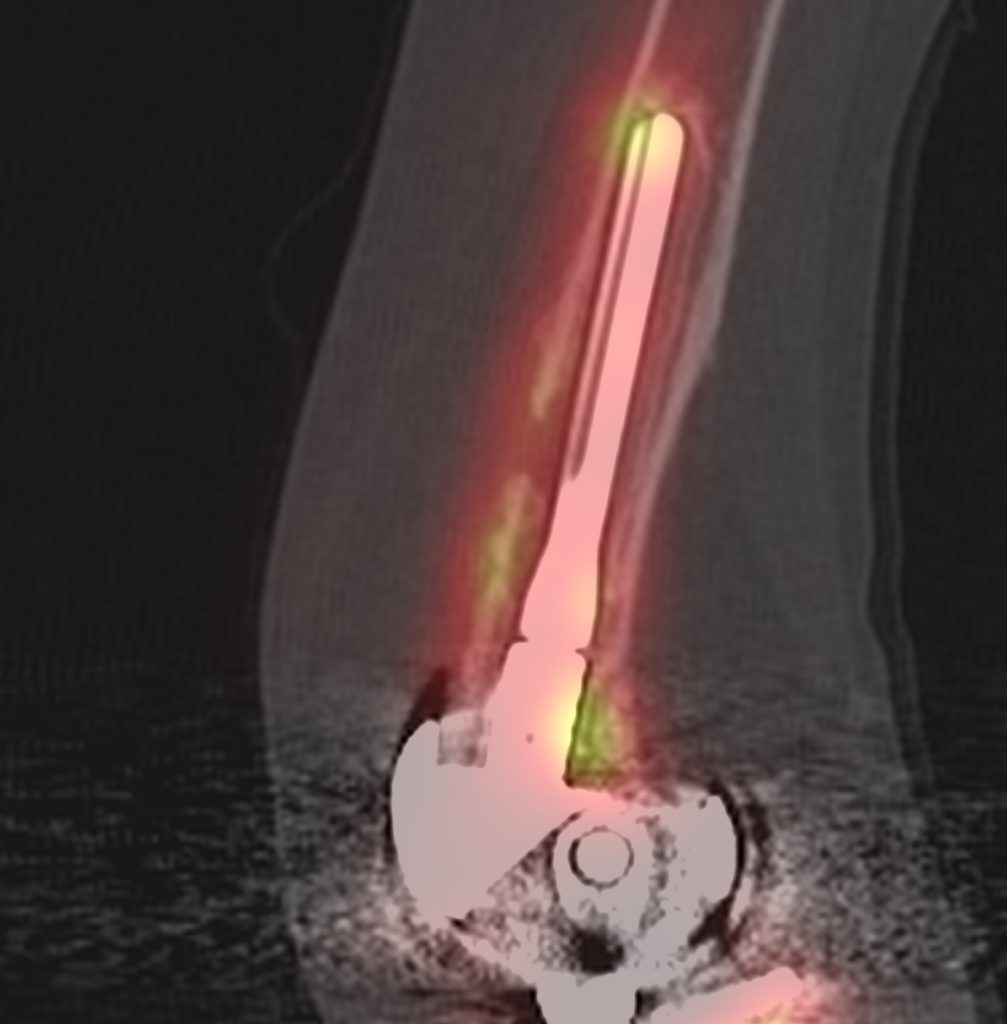
The tibial component is loose when there is focal increased tracer uptake at the sites of maximal mechanical stress; usually at the tip of the tibial component and at the contralateral tibial tray. Loosening of the femoral component is often associated with increased uptake adjacent to the posterior aspects of the condyles, adjacent to the bone prosthesis interface. The CT component will show a periprosthetic lucency that is greater than 2mm in width, with irregular margins, at the site of increased bone uptake.
Although traditionally increased blood flow on the dynamic and blood pool imaging suggests infection of the prosthesis, this is not reliable and in my experience, can often be seen with advanced aseptic loosening. If new bone formation is seen then infection should be considered in the differential.
Prosthetic Infection
Joint replacement infection is one of the most serious of complications with an incidence of 1.5–2.5% in primary joint replacements and up to 20% in revision joint replacements. The mortality rate is up to 3%.
Approximately one third of infections occur in the first three months after surgery, another third in the first year, and the remainder after a year.
It is difficult to differentiate aseptic loosening from infection as the inflammation due to infection is identical to that present in aseptic loosening. Whilst aseptic loosening can be treated with a single stage revision, patients with infected prostheses will usually require a two-stage revision. This means removing the infected prosthesis, followed by a course of antibiotics and subsequent revision after the infection has been completely cleared.
Bone tracer uptake around knee replacements are variable, and increased uptake can persist for many years after surgery. Up to two-thirds of infections occur within the first year when periprosthetic uptake is so variable. A negative bone scan has a high negative predictive value for infection and is useful even in the early post operative period.
Infected prostheses usually have increased activity in dynamic and blood pool phases throughout the bone surrounding the infected prosthesis. On SPECT-CT there is diffuse increased uptake around the bone prosthesis interface, with periosteal reaction, soft tissue oedema, soft tissue abscesses or joint effusions.
In equivocal cases, further imaging with white cell labelled scans combined with SPECT-CT can be performed. SPECT-CT with radiolabelled white cells shows increased diffuse uptake at the sites of infection. SPECT-CT can more accurately localise the site of infection around a prosthesis which helps in surgical planning.
Patellofemoral pathology
SPECT-CT can show increased uptake in the patellofemoral joint.
SPECT-CT is helpful for the diagnosis of several patellofemoral problems such as progression of patellofemoral disease, patellar maltracking, overstressing of the patella due to patella baja or femoral component malposition.
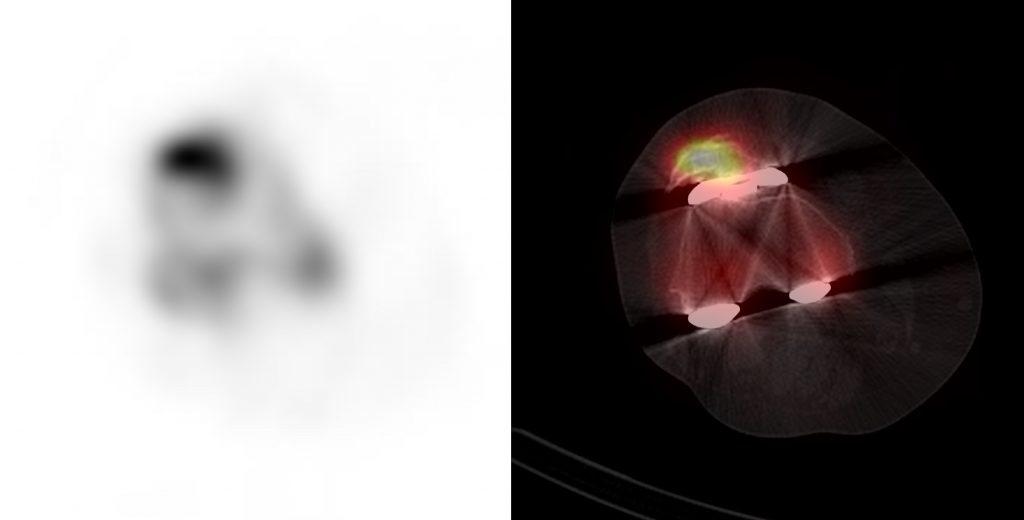
Focal increased uptake seen within the patellar facet is suggestive of patellofemoral degeneration. The position of the femoral component can result in abnormal loading on the patellofemoral joint. Internal rotation of the femoral component can result in loading on the lateral patellar rim. A flexed femoral component can cause increased uptake in the proximal patella due to overstuffing of the patellofemoral joint.
In patients who have undergone resurfacing of the patella, increased uptake around the patella resurfacing can indicate loosening of the prosthesis, infection, or mechanical overstressing.
Fractures
The incidence of total knee replacement periprosthetic fractures is low and has been reported as 0.3 - 5.5%.
Periprosthetic fractures can cause pain following surgery, lead to aseptic loosening, non-union, failure of osteosynthesis, infection, wound healing disorders and re-fractures. Bone scans can identify periprosthetic fractures, as increased bone turn-over associated with osteoblastic activation. However, SPECT-CT allows more accurate localisation of the fracture, along with providing information on prosthesis stability. One should look for cross-bridging of new cortical bone and new trabeculation of cancellous bone, which can be seen on CT. Increased bone uptake on SPECT indicates viability of the fractured component.