

Clinical presentation
This 18-year-old ballet student presented with chronic pain in the dorsal midfoot. There was no history of trauma. A bone SPECT-CT scan of the feet and ankles was requested by the orthopaedic surgeon to assess for the site of pain.
Key findings
Planar dynamic and blood pool phase images were unremarkable. This excluded an acute or inflammatory pathology.
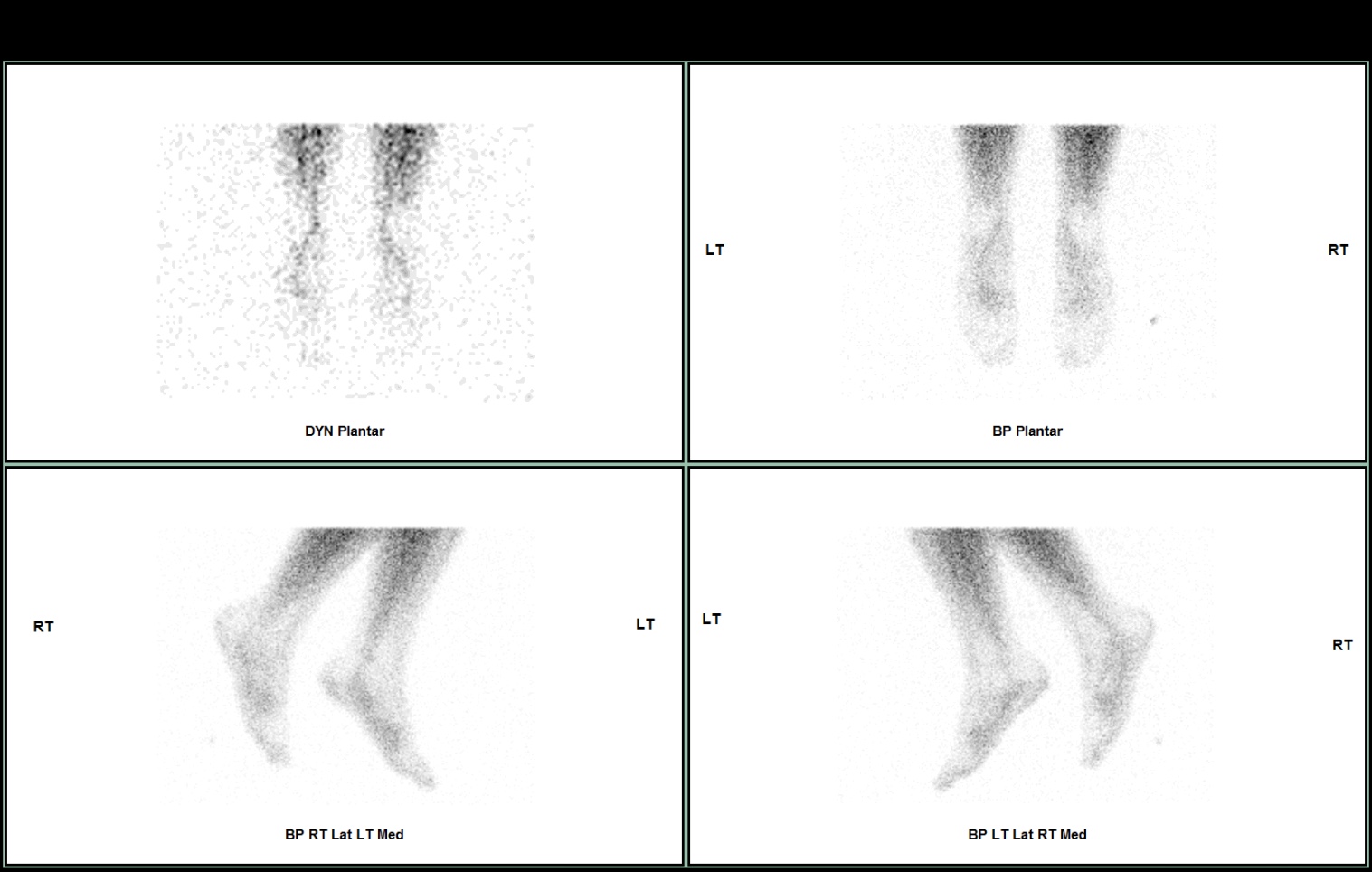

SPECT-CT shows focal increased uptake in the dorsal navicular bone, centred on a partially united fracture fragment. This was likely to represent a chronic stress injury due to dorsiflexion of the midfoot and is associated with an injury to the dorsal talonavicular ligament.
Diagnosis
Dorsal navicular avulsion fracture.
Navicular avulsion fractures
The midtarsal joint is defined by an S-shaped joint complex of the talonavicular and calcaneocuboid joint and supporting ligaments. The talonavicular joint is stabilised by the dorsal talonavicular ligament and the calcaneonavicular component of the bifurcate ligament.
The talonavicular joint is comprised of the convex anterior articular surface of the talar head which articulates with the concave articular surface of the navicular and the talar facets of the calcaneus. The dorsal talonavicular ligament is a broad capsular thickening of the talonavicular joint, extending from the dorsal talar neck and blending into the joint capsule. The dorsal talonavicular ligament is easily visualised on MRI. The ligament can be thickened, which may be due to traction on the ligament during normal weight bearing.

Avulsion of either the talar or navicular attachments of the talonavicular ligament often occur when there is ligamentous injury. Navicular avulsion fractures occur when there is excessive dorsiflexion with eversion or inversion of the foot. These can be well seen on the thin slice CT component of the SPECT-CT. In this case, the lack of increased vascularity on early phase imaging, suggests that the injury is longstanding. The uptake is due to incomplete union of the avulsion fracture.
If the talonavicular joint is stable then conservative management is followed for acute fractures, with patients returning to sport when pain free with provocative testing. For a direct traumatic injury, this may take up to 10 days of
immobilization followed by 2- 3 weeks of physiotherapy with arch supports.
Internal fixation is indicated for avulsion fractures involving > 25% of articular surface, tuberosity fractures with > 5mm
diastasis or large intra-articular fragment displaced or intra-articular fractures.


